

Asymptomatic Alveolar Swelling After a Tooth Extraction
Case Challenge Number: 64
Diagnostic Information
History of Present Illness Carmen is a 53-year-old female who presents for routine dental care. She is accompanied by her son who wants to take care of her after all of the years she was not able to take care of herself. Carmen moved to the United States from Mexico with her international banker husband in 1986. For 12 years she worked as an agriculture inspector in Ohio. In 1988 she lost her job and her husband abandoned her, took their life savings and moved back to Mexico. For the past 15 years she has been essentially living “on the street” in Ohio. Three months ago she moved in with her son who is determined to take care of her. She had an upper right molar extracted 2 weeks ago at a charity dental clinic due to a “crack.” She is currently in no discomfort. Medical History - Adverse drug effects: none
- Medications: metformin 1000 mg bid, losartan 50 mg bid
- Pertinent medical history: diabetes type 2, hypertension
- Pertinent family history: paternal - fatal stroke age 62; maternal - DM type 2, fatal MI age 71. No siblings
- Social history: denies alcohol, tobacco, and recreational drug use Clinical Findings Extraoral examination reveals normal TMJ function, no facial muscle tenderness, and no cervical lymphadenopathy. Intraoral examination reveals a normal healing extraction site #3, and missing #4 and #5. There is a distinct firm ovoid expansion of the alveolar process in the area of #4-5 (Figures 1 and 2). The occlusal aspect of the lesion is slightly ulcerated and exhibits an uneven pebbly surface. There is no pain on palpation. A panoramic radiograph reveals increased tissue density with unusual osseous expansion in the area of #4-5 (Figure 3). Incidental periradicular radiolucencies are also noted on #11 and on the mesial root of #19. An incisional biopsy was performed and the specimen was submitted for histologic assessment.

Figure 1. Visible enlargement alveolar process in the right maxillary premolar area.

Figure 2. Ovoid alveolar mass with a pebbly surface and focal ulceration.
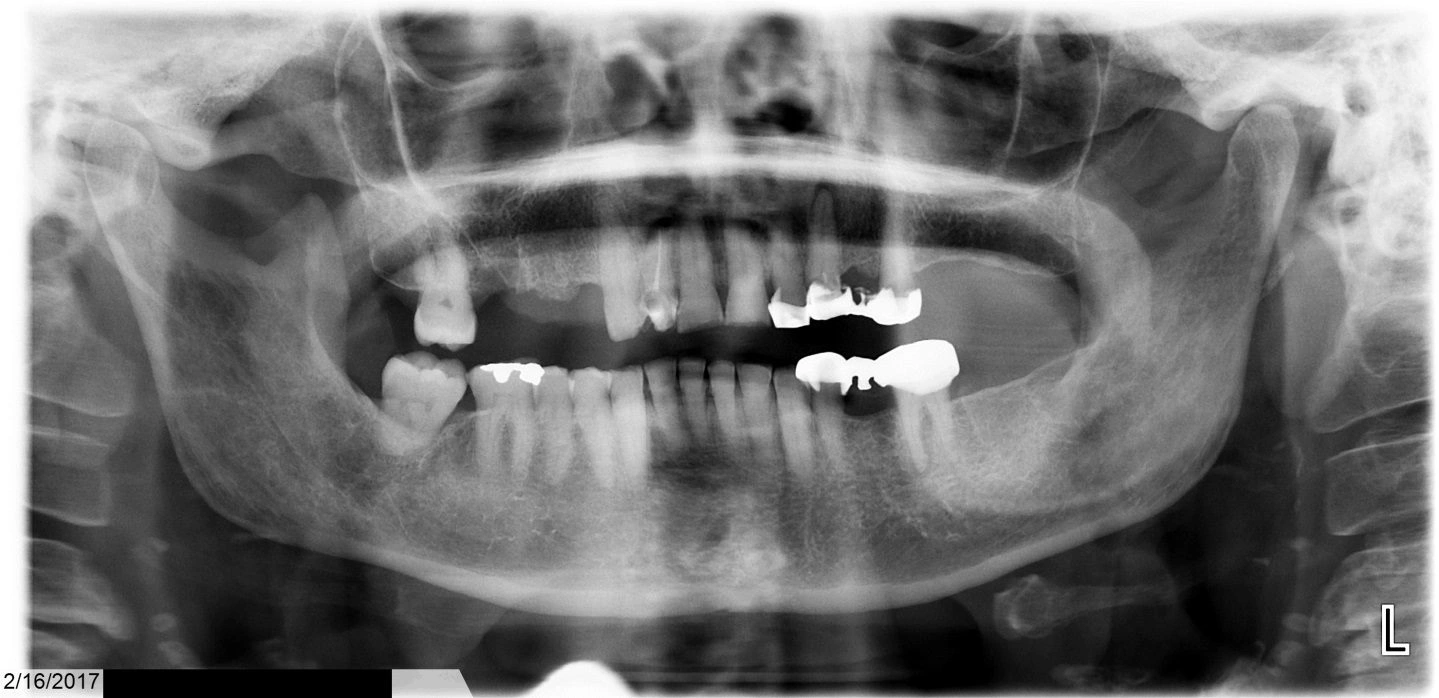
Figure 3. Increased tissue density with unusual osseous expansion in the area of #4-5.
Histopathologic Findings The histopathologic examination reveals infiltrating cords and islands of atypical squamous epithelium arising from dysplastic surface mucosa. The supporting fibrous connective tissue is well vascularized and contains a chronic inflammatory infiltrate. The epithelial cells displays pleomorphic round to oval shaped nuclei with finely dispersed to vesicular chromatin, prominent nucleoli, increased nuclear to cytoplasmic ratios, and pink focally, dyskeratotic cytoplasm. There are numerous abnormal mitotic figures and focal single apoptotic cells.
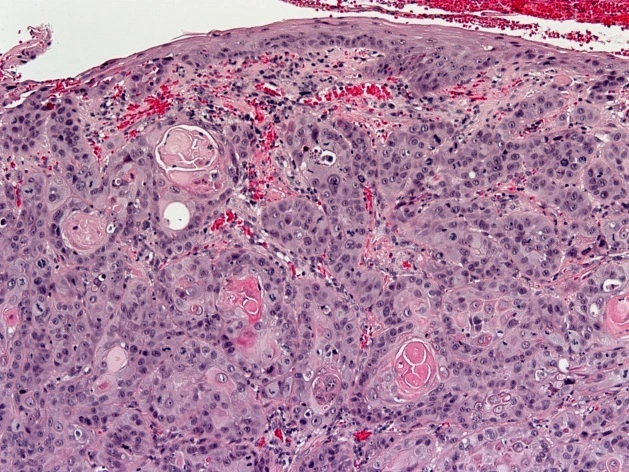
Figure 4. Low power histologic image showing invasive cords and islands of squamous epithelium extending into chronically inflamed fibrous connective tissue. The surface mucosa is dysplastic.
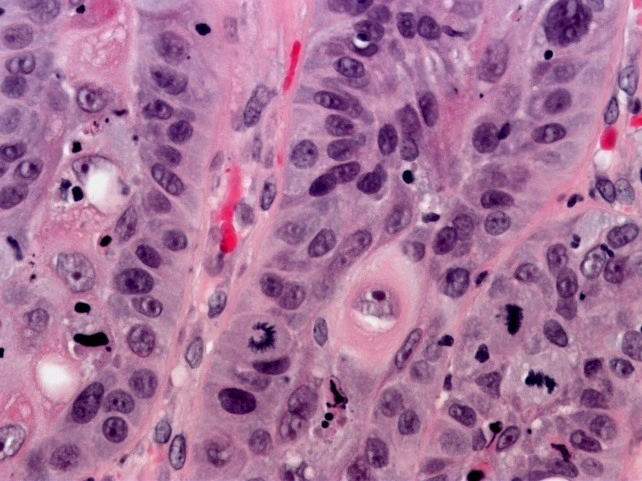
Figure 5. High power histologic image showing atypical epithelial cells with pleomorphic round to oval shaped nuclei, finely dispersed to vesicular chromatin, prominent nucleoli, increased nuclear to cytoplasmic ratio, and pink focally dyskeratotic cytoplasm. There are interspersed abnormal mitotic figures.